Dizziness, Dysequilibrium and Vertigo
From an ENT perspective dysequilibrium refers to a sensation of being off-balance or veering, similar to the sensation when one steps off a boat. Vertigo refers to a sensation of rotation, either of one's self spinning or the world spinning around them. Diseases of the ear affecting balance function normally but not exclusively cause vertigo.
Balance is a complex phenomenon that involves the eyes, ears, neck and brain. Problems in any of these areas can cause balance disturbance of one degree or another.
Common conditions
Benign Paroxysmal Positional Vertigo (BPPV)
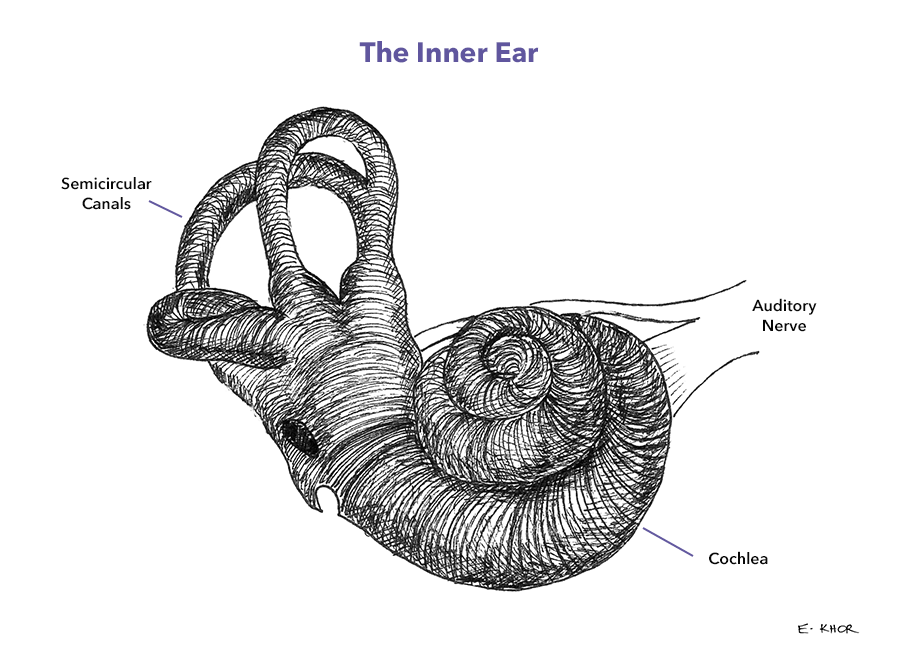
The inner ear contributes to balance by measuring head rotation and the direction of gravity. There are three semicircular canals on each side at 90° to each other. As the head turns in various planes the fluid moves through these canals and the flow is detected allowing rotation to be measured. There is another part of the inner ear that has heavy crystals hanging in the fluid. These are used to measure the direction of gravity.
If these crystals or other particles end up in the semicircular canals they cause false signals of rotation from the affected semicircular canal and BPPV results. The symptoms are a feeling of spinning when tipping the head back, down or most commonly rolling over in bed. The symptoms are brief.
Most resolve spontaneously but also do very well with a particle repositioning manoeuvre and often physiotherapy.
Meniere’s syndrome
This is a condition caused by a disturbance of the pressure and/or flow of fluid in the inner ear. The exact cause is unknown and in reality there are probably multiple causes.
It is characterised by recurrent attacks of true rotational vertigo lasting several hours typically. The episodes are often associated with pressure in the ear, worsening of tinnitus and a low-frequency hearing loss. That said the symptoms can be quite variable. The frequency and severity of attacks is also highly variable. There is a tendency over time for the attacks to become less frequent but for the hearing loss to persist.
Treatment can be difficult. It may include;
- medications
- injections of medications such as steroids or gentamicin into the ear
- more invasive surgery for refractory cases
- hearing aids if required and occasionally Cochlear implants
Evaluation
Meniere’s and BPPV are only two of the more common causes, there are many others.
Evaluation of these types of problems requires a discussion of the symptoms along with examination of the ears and neurological function. Frequently detailed audiological investigations are also needed. These can be performed at ENTSA, see Audiology Services
MRI and other investigations may be required.