Cochlear Implants and Bone Conduction Implants
Cochlear Implants
A cochlear implant is an implantable medical device used to reinstate useful hearing in people with moderate, severe or indeed profound bilateral or unilateral hearing loss.
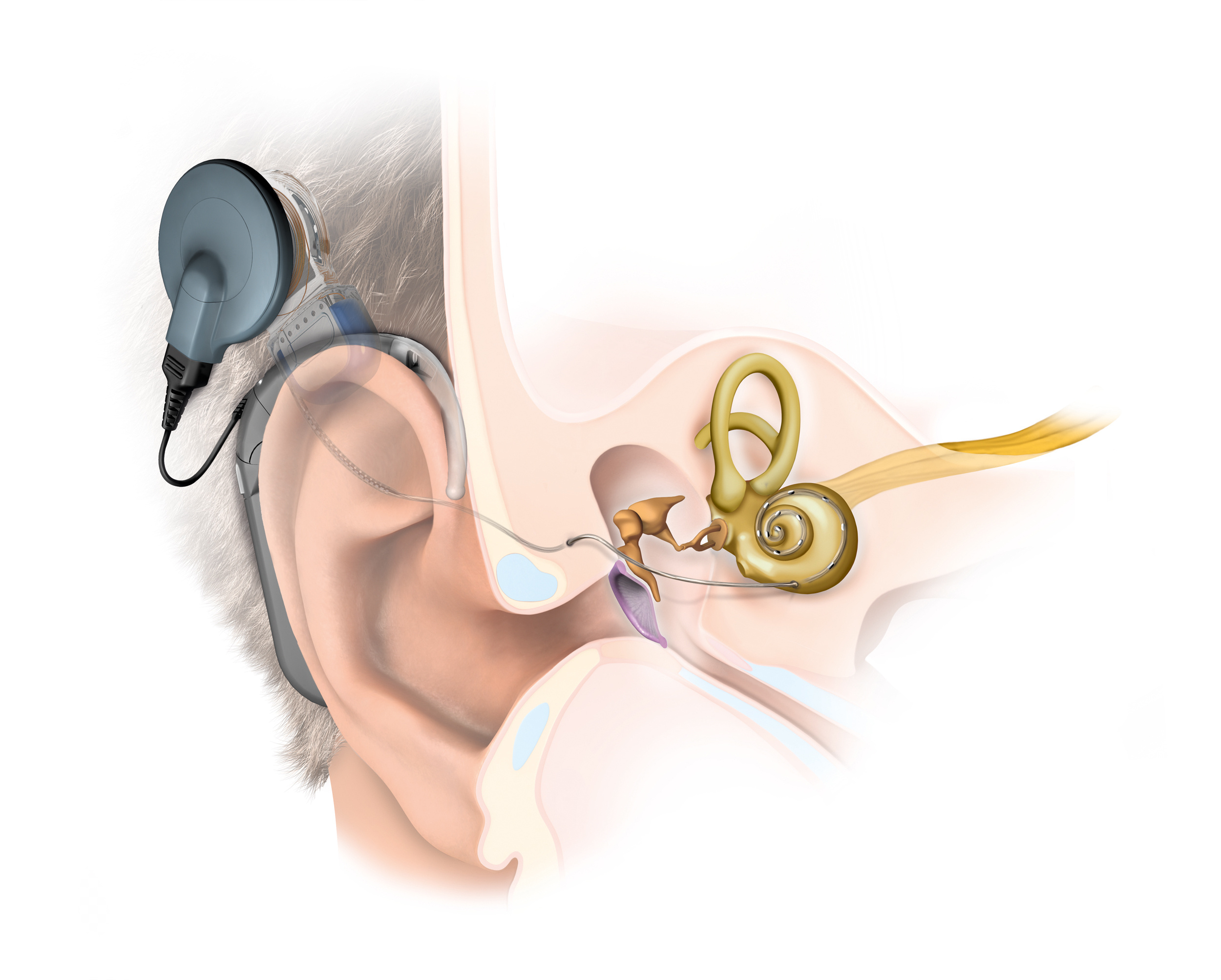
There are two main components to a cochlear implant, an internal and an external component.
The internal component
The internal component is surgically implanted. It consists of an electronics package that sits under the skin well behind the ear. It has an electrode array that is delicately inserted into the inner ear.
The external component

This is also known as a speech processor and sits on the ear similar to a conventional hearing aid. It transmits sound information to the internal component via a coil that self locates magnetically.
How they work
The external component or speech processor detects speech and other sounds and breaks each sound down into its component frequencies. This information is then transmitted to the internal component.
The electrode array inside the inner ear has many individual electrodes spaced out along the inner ear. The nerve fibres of the inner ear for each frequency are located in a predictable pattern. It is therefore possible for the implant to stimulate the appropriate nerve fibres for each frequency heard with the appropriate intensity.
A cochlear implant does not restore normal hearing. In the vast majority of cases however hearing, particularly speech perception is significantly improved.
Who are they for?
The technology of cochlear implants has improved rapidly over the last 10 years. In the early days cochlear implants were only for people with near total bilateral hearing loss. As the technology has improved it has been found that people with less severe hearing losses benefit as well.
Indeed in many cases current technology allows for cochlear implantation to be performed with good preservation of the residual natural hearing in the implanted ear. With older implants this was not the case and the recipient was totally reliant on hearing from the cochlear implant. The combination of residual natural hearing with the implant hearing works very well.
More recently it has been found that cochlear implants can also be of benefit to people with normal hearing in one ear and a significant loss in the other. In the past this was not the case and to be a candidate for cochlear implantation one needed bilateral hearing loss. Nowadays cochlear implantation may be a viable option for people with moderate to severe single sided deafness. In single sided deafness a cochlear implant will improve speech perception in noise, sound localisation and often gives a fuller richer hearing experience.
In summary then a cochlear implant may be a possibility in either single sided or bilateral significant hearing loss. They are usually only considered when conventional hearing aids have been tried and provide little or no benefit.
To decide whether implant is appropriate requires detailed testing with our cochlear implant audiologists, particularly to assess functional hearing. This involves testing for speech perception with and without hearing aids . If speech perception is relatively poor then a cochlear implant may well be good option.
Much more information about cochlear implants and candidacy can be found at www.sacic.com.au , the website for the South Australian Cochlear Implant Centre where I am a director and surgeon.
Also see:
The Operation
Cochlear implants are performed in hospital under general anaesthesia. A 5 cm or so incision is made behind the ear. It is performed using a high-powered microscope.
The bone behind the ear is called the mastoid. Using a drill this area is opened and the middle ear space is entered from behind, preserving the eardrum and skin of the ear canal. Once in the middle ear the inner ear is identified and opened carefully. The electrode array is gently advanced into the inner ear or cochlea. The electronics package is tucked in the pocket behind the mastoid and above the ear. The wound is then closed and a dressing and bandage applied.
The procedure generally takes between one and two hours.
After surgery
In Hospital
In most cases a one-day stay post-operatively is the norm. This is to allow for administration of intravenous antibiotics. It is also not uncommon to be a little off-balance for a few days.
Discharge from hospital
After 24 hours most people are well enough to go home. I will not send people-however until they are well enough do so.
Activity and return to work
Generally a week at home recuperating and resting is advised, thereafter a return to normal activities should be fine.
Pain relief
Pain is not a major feature in most cases. Paracetamol is normally sufficient however panadeine forte is also prescribed in case it is required.
Other medications
I normally also prescribe antibiotics to be used for one week.
Telemetry
Either during the operation or a few days after the surgery a telemetry check is performed. This is a simple process whereby the implant is connected to a computer to check all electrodes are functioning normally.
Switch on
2 to 3 weeks after the surgery the process of switching on begins. This process takes several weeks and involves programming the device over a number of visits to the audiologists.
Postoperative instructions
You will be given instructions for care upon discharge. These are also available to download here. At discharge you will also be given a post-operative appointment and my mobile phone number.
Bone Conduction Implants
Cochlear, Medel and Oticon all have bone conduction devices in there range of devices for hearing rehabilitation. Whilst they vary in design and method they all essentially rely on the principle that the bones of the skull are excellent conductors of sound. As such they all employ a vibrating sound source (a transducer) in one form or another. Once sound waves pass to the bone they travel efficiently to the inner ear where they are perceived in the same way as sound waves entering via the ear canal.
Each of these devices whilst similar have advantages and disadvantages. As such thay all have a role depending on the clinical situation. Personal choice is also important in final selection.
Bone Conduction Implants by Cochlear
Cochlear have three devices available. The BAHA connect,BAHA attract and the Osia. In all three an osseo-integration screw is used to connect the device to the bone thus allowing efficient transfer of sound. The BAHA devices have external transducers whereas in the Osia the transducer is under the scalp.
The BAHA Connect
An abuttmennt is attached to the osseo-integration screw. This abuttment protrudes through the skin and the speech processor containing the transducer clips on.
The BAHA Attract

This device differs from the traditional BAHA above in that the skin is intact with no abutment protruding through the skin. Instead a magnet is attached to the skull and the skin closed over it. Once the wound has healed the same speech processor can be attached using a magnet. This has the advantage of having a lower risk of infection and a lot less maintenance. The sound transmission however is not quite as efficient.
The Osia
This newer device again uses an osseo-integration screw but unlike the BAHA devices the transducer is attached directly to the screw and in inner the scalp. Nothing protrudes through the skin and a flatter smaller external device can be used as it no longer needs to house the transducer.
More information abouth these devices can be found at the South Australian Cochlear Implant Centre
https://www.sacic.com.au or cochlear.com
The Bonebridge by Medel

In this device the tranducer is fitted into the mastoid behind the air. The mastoid is a predominantly air filled space within the skull. A recess is drilled into the mastoid to house the transducer and two screws attach its small wings to the skull. The transducer floats free and the screws transmit the sound waves to the bone. Nothing protrudes through the skin so maintainence is minimal.
more information can be found here;i
https://www.medel.com/int/bonebridge/
When can they be considered?
These devices can be very useful in a number of situations.
They are particularly useful when there is reasonable residual hearing but conventional hearing aids cannot be used due to poor fit or frequent infections when hearing aids are used.
They can also be useful in severe single sided deafness. In this scenario they are actually transmitting sound to the normal ear on the other side. This does not create true stereo hearing but gives 360° sound awareness. They will probably be used less in this situation as cochlear implants are now being offered for single sided deafness.
It is a complex area and the choice between these different devices will depend on the individual, their residual hearing, and their anatomy and individual preferences.
As such the decision will be reached after several in-depth consultations both with myself and also our implant audiologists.